Know about your bladder and kidneys
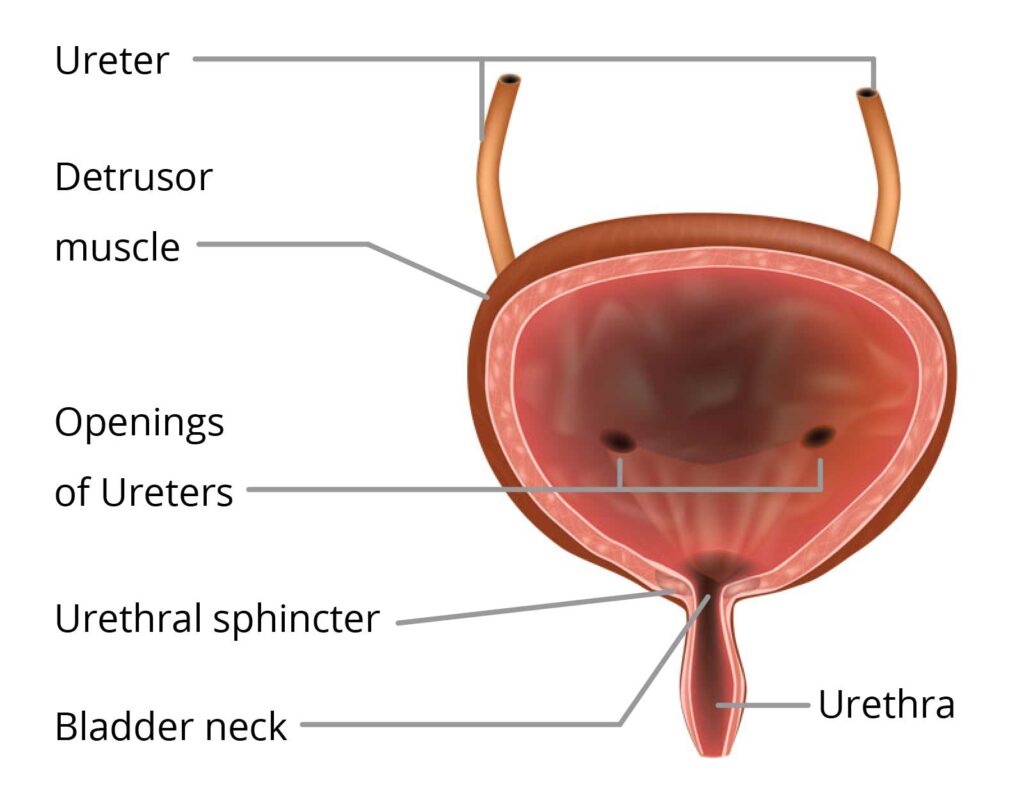
How the bladder normally works
Urine forms as the blood filters through the kidneys. The urine drains down through tubes called ureters for storage in the bladder.
When your bladder is full of urine, it causes the bladder wall muscles to stretch. Nerve impulses or messages travel from your bladder to your brain via your spinal cord. You become aware of how full your bladder is and can decide whether to urinate or to wait until later. You have control over when you go to the toilet.
If you choose to pass urine, your brain sends a message down the spinal cord to the bladder to contract its muscles. As the bladder contracts, the bladder outlet or sphincter muscles relax for coordinated emptying. The urine passes through the urethra to outside of the body.
If you choose not to pass urine, your bladder will keep holding urine until you decide to go to the toilet.This is how your bladder works to store and then pass urine when you do not have a spinal cord injury.

Effects of a spinal cord injury
After injury, spinal nerves carrying messages from the brain to your bladder do not work in the usual way. This type of bladder is often referred to as a neurogenic bladder.
There are two main types of neurogenic bladder depending on where your injury is:

T12
Overactive or spastic (hyperrefeflexic) bladder
At and above T12 vertebral level (sacral nerves are intact)

- Bladder muscles get very excited due to lack of control by the brain.
- Bladder holds less urine and bladder muscle spasms as bladder fills up.
- Results in high pressure as the bladder fills with more frequent but poorer urination.
Underactive or flaccid (areflexic) bladder
Below T12 vertebral level (sacral nerves are damaged)

- Bladder muscles are sluggish or do not work due to damage to the sacral nerves.
- Loss of the ability to contract and bladder is easily stretched.
- Bladder can overfill and leak.
Note: Due to the level of spinal cord injury, some bladders may have a mixed pattern, with some features of both main types.
When you have a neurogenic bladder, you may experience problems with storing urine and/or completely emptying your bladder.
This is a common problem in an overactive bladder that empties too soon and often without any warning as it fills with urine. This usually occurs in people with spinal cord injury above the T12 level.
It can cause:
- Urine to leak (incontinence)
- Passing urine more often
- A strong sense of need to pass urine (urgency)
- High back pressure on the kidneys as the bladder is filling up.
Leakage of urine can also occur in an underactive bladder due to overflow (see ‘Problems with emptying your bladder’).
Your doctor may recommend taking an oral tablet to relax your bladder. The most common anticholinergic medication is Oxybutynin (sold as Ditropan). If tablets do not work, a Botulinum toxin injection into the bladder wall may help. This aims to increase the urine storing capacity of an overactive bladder.
This is a common problem in an underactive bladder that does not empty well and retains urine. It can stretch and fill up too much, causing urine to leak when it overflows.
Failure to empty well can also occur in an overactive bladder. This is due to the bladder outlet or sphincter muscles spasming as the bladder empties. This can cause difficulty inserting a catheter or prevent emptying of the bladder completely. There is an increased chance of infection if the amount of urine remaining in the bladder is 100ml or more.
Your specialist may recommend taking an oral tablet (alpha-adrenergic blocker) to relax your sphincter muscles. Botulinum toxin injection into the sphincter muscle or surgery called a sphincterotomy are other options.
How Does Spinal Cord Injury Effect the Bladder?
How people manage their bladder
In 2015 the Rural Spinal Cord Injury Project surveyed 681 people living with spinal cord injury in rural NSW. These were their findings on the most common methods people used for managing their bladder.
Ways people manage their bladder

Ways to empty your bladder
There are three common ways to empty your bladder:
- Intermittent catheterisation
- Permanent catheterisation
- Reflex voiding – reflex voiding is no longer recommended due to associated risks.
The choice of method depends on factors such as level of injury, lifestyle and gender.
The two most common methods are explained below.
Intermittent catheterisation
- This is the preferred method for people with enough hand function.
- Using this method, drain the bladder for 5 minutes or so by inserting a catheter at regular intervals.
- Drain the bladder every 4 to 6 hours, but this depends on the amount and type of fluid you drink.
- Recommended catheter size is 14, but for people with prostrate problems, use 16 gauge instead.

Important Notes
Intermittent catheterisation is not recommended when you have:
- Abnormal urethral anatomy (such as stricture, false passages, and bladder neck obstruction)
- Reduced bladder capacity (less than 200ml)
- Poor decision-making, lack of motivation, inability or unwillingness to adhere to the catheterisation time schedule
- Persistently high fluid intake
- Adverse reaction to passing a catheter into the genital area multiple times per day
- Tendency to develop episodes of autonomic dysreflexia with bladder filling despite treatment.
What does research tell you?
- Clean intermittent self-catheterisation is the preferred method of bladder management for people with spinal cord injury who have enough hand function.
- The use of single-use hydrophilic catheters lowers the risk of a urinary tract infection.
Permanent catheterisation
There are two types of permanent catheterisation:
- Indwelling catheter (IDC): this catheter drains urine from your bladder via the urethra. Recommended catheter size is 12 to 16 gauge.
- Suprapubic catheter (SPC): this type of catheter is inserted into the bladder through a small cut in the lower abdominal wall. Recommended catheter size is 18 to 24 gauge.
In both types, there is continuous drainage with the urine draining into a urinary drainage bag.

Important Notes
Reflex voiding involves passing urine by triggering an automatic response using a technique like tapping over the bladder or stroking the inner thigh.
Reflex voiding is no longer recommended because of the long-term risk of high pressure being placed on the kidneys as the bladder fills against resistance which may lead to kidney failure in the long term.
Reflex voiding may also lead to other potential problems such as catheter leakage or skin breakdown of the penis. Using a condom catheter may result in recurrent symptomatic UTI, poor bladder emptying, and autonomic dysreflexia.
What does research tell you?
- People with an overactive bladder using a permanent suprapubic or indwelling urethral catheter are recommended to take an anticholinergic medication.
- Reflex voiding should no longer be used because it can cause too much pressure in the bladder and damage to the kidneys.
Selecting a catheter
- Your level of injury
- Degree of hand function and dexterity
- Your lifestyle (includes school, work and social activities)
- Cost and ease of use
- Other existing medical conditions
- The availability and expertise of your caregiver.
Do you know?
A single-use, disposable catheter may help reduce the chances of bladder infection, especially with a catheter tip that remains sterile (closed ‘no touch’ system). This type of catheter may be preferred, particularly when you are experiencing frequent urinary tract infections.
Advantages and disadvantages of different types of catheters
Type of management | Advantage | Disadvantage |
|---|---|---|
Intermittent catheterisation | Reduced infection. | Usually need to take anticholinergic medications which are costly
and you may require assistance with insertion. |
Permanent catheter | Reduces pressure in your bladder and often recommended with limited hand function.
Convenience and less
caregiver assistance. | Increased risk of infection, problems with blockage.
May need to access external providers for catheter changes. |
Type of management | Intermittent catheterisation |
|---|---|
Advantage | Reduced infection. |
Disadvantage | Usually need to take anticholinergic medications which are costly
and you may require assistance with insertion. |
Type of management | Permanent catheter |
|---|---|
Advantage | Reduces pressure in your bladder and often recommended with limited hand function.
Convenience and less
caregiver assistance. |
Disadvantage | Increased risk of infection, problems with blockage.
May need to access external providers for catheter changes. |
Bladder management supplies
Eligibility for continence supplies
You may be eligible (certain criteria apply) for continence supplies under various schemes, as summarised in the table below:
Schemes/ Programs | Under 65 years | 65 years and over |
|---|---|---|
National Disability Insurance Scheme (NDIS) | $ | |
My Aged Care | * | |
Continence Aids Payment Scheme (CAPS) | ||
EnableNSW | ||
icare NSW# |
$ Unless you have accessed scheme prior to turning 65 years.
* Your package may not include your bladder supplies.
# For eligible participants only.
Please talk to the relevant organisation/s or your healthcare provider for details about eligibility and further information.
Schemes/ Programs | Website | Contact details |
|---|---|---|
National Disability Insurance Scheme (NDIS) | www.ndis.gov.au/people-disability | 1800 800 110 |
My Aged Care | www.myagedcare.gov.au | 1800 200 422 |
Continence Aids Payment Scheme (CAPS) | www.bladderbowel.gov.au/caps | 1800 239 309 |
EnableNSW | www.enable.health.nsw.gov.au | 1800 362 253 |
icare NSW | www.icare.nsw.gov.au | 1300 738 586 |
Schemes/ Programs | Contact Details |
|---|---|
National Disability Insurance Scheme (NDIS) | www.ndis.gov.au/people-disability 1800 800 110 |
My Aged Care | www.myagedcare.gov.au 1800 200 422 |
Continence Aids Payment Scheme (CAPS) | www.bladderbowel.gov.au/caps 1800 239 309 |
EnableNSW | www.enable.health.nsw.gov.au 1800 362 253 |
icare NSW | www.icare.nsw.gov.au 1300 738 586 |
The details in this table were last verified on 28th April 2022